





➣ By Brenda K. Wiederhold

The Client wears a headmounted display with small monitors to receive both visual and auditory cues
What if the thought of entering the enclosed space of an elevator terrified you so badly that you decided to climb the seven flights of stairs to your doctor’s office? Or imagine having to send regrets to your best friend’s wedding because you could not stand the idea of mingling at the reception. Though fear and anxiety are a normal part of the human experience, for some these feelings are so intense that they can severely impact everyday life. For these people, there are various treatments that can offer hope, some with traditions stretching for hundreds of years, and others newly arrived, seemingly from the realm of science fiction.
Anxiety disorders, as a group, are the most common mental illnesses in the world. According to a 2007 study by the Anxiety Disorder Resource Center, anxiety disorders affect approximately 1 in 4 people worldwide at some point in their lives. The Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) lists phobias (specific phobias, social phobia, and agoraphobia), panic disorder, obsessive-compulsive disorder, posttraumatic stress disorder and generalized anxiety disorder under the broad category heading of Anxiety Disorders. This group of disorders does not distinguish between age, sex, or race, afflicting those from all walks of life. Not only adults, but also children and adolescents can develop anxiety disorders.
Most people experience feelings of anxiety before an important event such as a business presentation, big exam, or first date. Anxiety disorders, however, are illnesses that fill people’s lives with overwhelming anxiety and fear that are chronic, unremitting, and can grow progressively worse. Tormented by obsessive thoughts, flashbacks of traumatic events, panic attacks, nightmares, or countless frightening physical symptoms, some people with anxiety disorders may even become housebound. Groups around the world are, however, advancing the treatment of these conditions through the use of virtual reality (VR) therapy.
VR exposure therapy immerses an individual in a computer-generated world where various stimuli related to the phobia may be “experienced” three-dimensionally. The client wears a head-mounted display with small TV monitors and stereo earphones to receive both visual and auditory cues. In careful, controlled stages, the client is exposed to experiences that elicit higher levels of anxiety. Each stage can be repeated until the client is comfortable with the experience and satisfied with the response.

VR environment for treating aviophobia
Specific Phobias
Phobias are the most common psychiatric disorder, more common than alcohol abuse, alcohol dependence, or major depression. A specific phobia is defined as an intense and persistent fear that is considered excessive or unreasonable in response to a situation. Specific phobias include fear of flying, spiders, heights, thunderstorms, public speaking, blood, etc. Exposure to the phobic stimulus consistently provokes an anxious reaction, which may take the form of a situationally predisposed panic attack. Adults recognize that their fear is excessive and unreasonable, but are unable to control it. Children may or may not have any insight into the fact that their fear is excessive. In both adults and children, the feared object or situation is usually avoided or anticipated with dread. The phobia is diagnosed when one’s fear, or evasive actions to avoid the feared situation, interferes with daily routine, employment, or social life.
Over 200 phobias have been identified and named, falling into five different subtypes:
- Animal Type, which generally has a child – hood onset and includes fear of insects or other animals.
- Natural Environment Type, which inclu – d es fear of heights, water, and storms and generally has a childhood onset.
- Blood-Injection-Injury Type, including fear of invasive medical or dental procedures such as receiving an injection, giving blood or seeing blood or an injury. This phobia subtype is often characterized by fainting.
- Situational Type, which includes fear of flying, bridges, elevators, driving, or enclosed places. The age of onset is either during childhood or in the mid-20s. This is the most frequent subtype seen in adults.
- Other Type, which includes fear of falling down when away from walls, fear of vomiting or choking, fear of contracting an illness, fear of loud sounds, and fear of costumed characters.
The most common treatment for specific phobias is exposure therapy. This exposure was typically done either in real-life (in vivo) or imaginally (in vivo) prior to VR. However, in vivo exposure is not always convenient, safe, or cost-effective (e.g. fear of flying, fear of driving), and in vitro is often difficult as only 15% of individuals are able to imagine the feared situation vividly enough to evoke the anxiety response necessary for successful treatment. That’s where virtual reality (VR) steps in. In Virtuo exposure provides all of the stimuli needed for successful treatment while at the same time allowing therapy to take place in a secure, controlled environment. Studies around the globe have shown that VR for specific phobias has approximately a 92% success rate in just 8-12 one-hour sessions. In addition, by adding physiological monitoring and feedback to the VR protocol, relapse rate and both short and longterm treatment gains may be further improved.
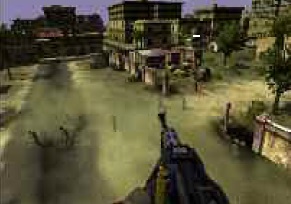
VR environment for treating posttraumatic stress disorder
Social Phobia
Social phobia, or social anxiety, is a disorder characterized by excessive self-consciousness and overwhelming anxiety in everyday social situations. People with social phobia have a persistent, intense, and chronic fear of being watched and judged by others and of being humiliated or embarrassed by their own actions. Their fear may be so severe that it interferes with work, school, and other ordinary activities. While many people with social phobia recognize their fear is excessive or unreasonable, they are unable to overcome it. They often worry for days or weeks in advance of the dreaded situation.
Social phobia may involve only one type of situation (such as a fear of speaking in formal or informal situations, or eating or drinking in front of others) or, in its most severe form, it may be so broad that a person experiences symptoms almost any time they are around other people. Social phobia can be very debilitating and can even prevent an individual from going to work or school. Many people with this illness have a hard time making and keeping friends.
Physical symptoms often accompany the intense anxiety of social phobia and may include symptoms of anxiety such as profuse sweating, trembling, blushing, difficulty talking and nausea or other stomach discomfort. These visible symptoms heighten the fear of disapproval and the symptoms themselves can become an additional focus of fear. Fear of symptoms can create a vicious cycle: as people with social phobia worry about experiencing the symptoms, the chances of developing the symptoms increase. Social phobia often runs in families and may be accompanied by co-morbid disorders such as depression or alcohol dependence.
Research has shown two main forms of effective treatment: medication and cognitive- behavioral therapy (CBT). A main component of CBT is exposure therapy, which involves helping patients gradually become more comfortable with situations that frighten them. The exposure process often involves three stages. The first is introducing the individual to the feared situation. The second level is to increase the risk for disapproval in that situation so the patient builds confidence and can handle rejection or criticism. The third stage involves teaching the patient techniques to cope with disapproval. In this stage, the individual is asked to imagine his/her worst fear and is encouraged to develop constructive responses to this fear and any perceived disapproval.
All three stages of exposure can be accomplished in vivo, in vitro, or in virtuo (VR). However, using VR provides certain advantages. First, therapy is carried out in the privacy of the therapist’s office. Second, the therapist can more carefully control the reactions of the people with which the patient is interacting. And most importantly, treatment can progress at the user’s own pace. It allows each session to be customized to the individual receiving treatment.
Panic Disorder
Panic disorder is characterized by unexpected and repeated episodes of intense fear (called panic attacks) accompanied by physical symptoms that may include shortness of breath, dizziness, chest pain, heart palpitations, or abdominal distress. These sensations often mimic symptoms of a heart attack or other life-threatening medical condition. As a result, the diagnosis of panic disorder is unfortunately often not given until extensive and costly medical procedures fail to provide an alternate diagnosis or relief.
Many people with panic disorder develop intense anxiety between episodes. It is not unusual for a person with panic disorder to develop phobias about places or situations where panic attacks have occurred, such as in supermarkets or other everyday situations. As the frequency of panic attacks increases, the person often begins to avoid situations where they fear another attack may occur or where help would not be immediately available. This avoidance may eventually develop into agoraphobia, an inability to go beyond known and safe surroundings because of intense fear and anxiety.
Appropriate treatment by an experienced professional can help reduce or prevent panic attacks in 70% to 90% of people with panic disorder. Treatment for panic disorder often includes medications and CBT. CBT teaches people how to view panic attacks differently and demonstrates ways to reduce anxiety. VR environments used to treat panic disorder involve exposing patients to feared situations (similar to those where they have experienced panic attacks) or to reproductions (interoceptive exposure) of the physical symptoms of panic attacks (e.g., shortness of breath, vertigo, and tunnel vision). These symptoms can be recreated in virtual environments with sound (pounding heart, fast breathing) or with visual effects (blurred or stretched images). Each of these exposures is accompanied by therapist- facilitated cognitive restructuring and coping skills.
Most patients show significant progress af ter approximately ten treatment sessions. Relapses may occur, but they can often be effectively treated with “booster sessions” or a short “refresher” course.
Obsessive-Compulsive Disorder
There are two sides to obsessive-compulsive disorder (OCD): obsessions and compulsions. Obsessions are thoughts, and compulsions are actions. The obsessions in OCD are repetitive and persistent, inappropriate and intrusive, and are impossible to suppress. These cause the sufferer significant distress and anxiety. Compulsions are repetitive behaviors or mental acts that the person applies based on rigid rules that they follow. The goal of these actions is to prevent a dreaded event or to lessen distress. They are, however, not really connected in a logical way to these events. Once the person completes a compulsive behavior, a sense of relief is felt. It is easy to imagine how these unwanted thoughts and disruptive behaviors cause disturbances and impair the sufferer from living everyday life. Not only are these rituals time consuming, but it is quite difficult to function socially while experiencing them.
OCD is most often treated with a combination of medication and exposure therapy with ritual prevention. Some medications have been found to have a significant effect on symptoms, but relapse rates upon medication cessation are extremely high if coping skills are not also learned prior to discontinuing medication. Research has revealed that VR is effective at inducing the anxiety response necessary for effective treatment to take place. The benefit of conducting exposure therapy with VR is that situations that trigger obsessions and compulsions can be experienced repeatedly, a necessary element of overcoming the repetition of OCD. In addition, this treatment can take place in the privacy of a therapist’s office, ensuring patient confidentiality. Though VR exposure therapy for OCD can take longer than for specific phobias, many patients experience some relief within the first few sessions.
Posttraumatic Stress Disorder
Many have heard the term “shell shock” in the context of soldiers returning from war. The condition’s technical name is Posttraumatic Stress Disorder (PTSD). PTSD can affect anyone who has experienced a traumatic event such as a motor vehicle accident, an assault, or anything that threatens a person’s life or physical integrity. Symptoms may range from increased anxiety or arousal to dissociation and flashbacks of the event, though the disorder may manifest differently in each individual.
Because PTSD has such varied symptoms, a combination of treatments is often necessary. Anxiety-reducing medications, antidepressants, support from friends and family, and CBT involving exposure can help with recovery. A recent Institute of Medicine study maintains that exposure is an important component to be included in treatment regimens. One type of exposure therapy that has often been used is imaginal exposure therapy, in which patients are asked to repeatedly imagine and retell their traumatic experience to their therapist. However, because one of the hallmarks of PTSD is an avoidance of reminders of the trauma, this is often difficult for some patients. Those who are unable to engage with their memories do not evoke an anxiety response during exposure, and these patients fail to improve. It is generally thought that this is due to lack of activation of the brain’s fear structure, where the trauma memories are stored. Since the structure is not activated, it is thought that the information stored is therefore not available to receiving “disconfirming” information (e.g., “there is no longer danger here”).
Virtual reality (VR) can solve the problem of avoidance and lack of good imagery abilities that plague some patients and prohibits successful alleviation of symptoms. By providing the patient with stimuli that engage multiple senses (audio, visual, tactile, and olfactory), the therapist does not have to rely on the imagination and willingness of the patient to create anxiety, but rather can provide stimuli directly to the patient at the touch of a button. In addition, because the virtual environment allows the therapist and patient complete control over the pace and duration of treatment sessions, the danger of overwhelming the patient with anxiety can be avoided, alleviating the patient’s anxiety at beginning treatment. In addition, many clinicians combine physiological monitoring and feedback with VR exposure. This has the added advantage of providing continuous monitoring of the patient’s heart rate, breathing rate and other physiological signals, allowing for an objective, real-time measurement of the patient’s condition to occur. This also can be used to teach the patient to visually understand when relaxation has been achieved. With this addition, the therapy can be further individualized to progress according to each individual patient’s needs.
VR exposure treatment has been performed for survivors of earthquakes, motor vehicle accidents, terror attacks and other various traumatic events. One of the most recent developments has been to use this treatment for those returning from Iraq and Afghanistan who are diagnosed with PTSD (www.vrphobia.com). The Virtual Reality Medical Center and Interactive Media Institute, have both received funding from various military and government organizations to develop virtual reality software and clinical protocols, and to provide treatment to both U.S.-based active duty and veteran populations as well as NATO coalition troops and continuing clinical education and training to psychologists and psychiatrists. Currently in use at over thirty installations in the U.S., systems are also now available in both Warsaw, Poland and Zagreb, Croatia. Psychologists and psychiatrists trained on the clinical protocols are now able to provide this innovative treatment to patients.
The VR programs recently established in Croatia and Poland will not only help patients, but will allow for the clinical investigation of determining the system’s crosscultural relevance. Some parts of the sys tem may be shown to be transferable across cultures whereas other portions may need to be re-configured to allow for cultural differences.
Conclusion
Virtual reality has made a significant impact on the way anxiety disorders are able to be treated. With increasing advancements in technology, and with the availability now to port many VR experiences over the Internet, the potential for improved psychological treatment of mental disorders is seemingly endless. With over 200 recognized anxiety disorders affecting one-fourth of the world’s population, the need for continued improvement of treatment availability is critical. With advanced technologies, psychology has the opportunity to rise to a new level, moving towards unprecedented heights to offer more affordable, more available healthcare to a larger portion of our society.
Brenda K. Wiederhold, Ph.D., MBA, BCIA
Virtual Reality Medical Center
www.vrphobia.com
frontoffice@vrphobia.com
 About Brenda Wiederhold
About Brenda Wiederhold
President of Virtual Reality Medical Institute (VRMI) in Brussels, Belgium.
Executive VP Virtual Reality Medical Center (VRMC), based in San Diego and Los Angeles, California.
CEO of Interactive Media Institute a 501c3 non-profit
Clinical Instructor in Department of Psychiatry at UCSD
Founder of CyberPsychology, CyberTherapy, & Social Networking Conference
Visiting Professor at Catholic University Milan.


