





➣ Rasheda Farid & Khodeza Begum
The growth of psychology as a separate field was not considered in Canada until the last half of the 19th century. The first psychology course was taught by Thomas Mucculloch at Dalhousie University in eastern Canada in 1838. Ten years after the establishment of the first psychology laboratory in Germany in 1879 by Wilhelm Wundt, James Mark Baldwin, one of Wundt’s students, founded the first psychology laboratory in Canada. Although individual psychology departments began expanding in the 1920s, it was not until the 1940s that psychology was truly separated from philosophy.
Overcoming Roadblocks:
Constitutional and Personal Attitudes
According to the Canadian constitution, individual provinces are responsible for the sector of mental healthcare, meaning the country does not have a supreme mental health strategy.
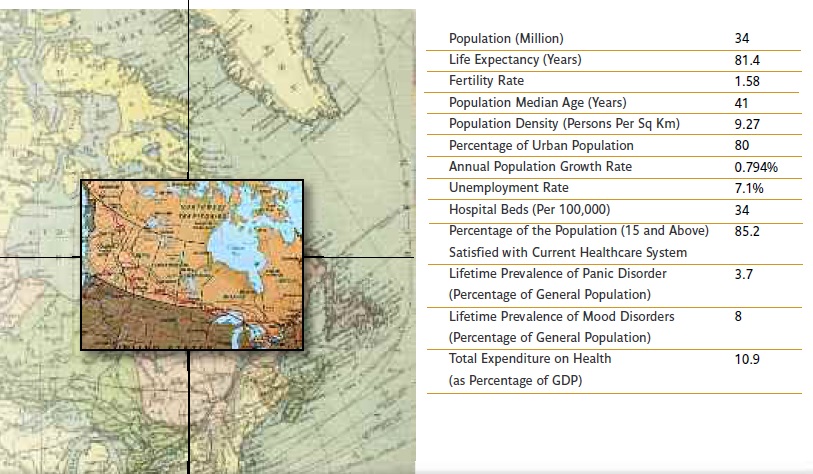
Researchers have estimated that almost one in every five Canadian adults will experience some type of mental illness in a year. However, many do not get proper treatment or have access to care. The quality and quantity of services available to those affected is insufficient to meet their need. Additionally, fear of stigma keeps many from seeking help, while others are unable to afford treatment.
The Canadian Senate Committee on Social Affairs, Science and Technology came to the conclusion that Canada was in critical need of a “profound transformation of the mental healthcare system … a genuine system that puts people living with mental illness at its center, with a clear focus on their ability to recover.”
A Step Forward for Mental Healthcare
The federal government, with the collaboration of provisional and territorial governments, announced the creation of the Mental Health Commission of Canada (MHCC) in 2007. Its mission was to hasten the development of a mental health strategy for Canada, acknowledging that all the jurisdictions had neglected mental health needs and were faced with the same challenges.
The MHCC developed a framework for a Mental Health Strategy between June 2007 and September 2009, aiming to increase awareness of mental health and structure an official strategy for the country to follow to properly address the issue as a unified nation.
The Structure and Process
The Commission felt it was important to engage a wide range of people in order to develop the framework, including those suffering from mental health issues, their families and caregivers, advocates, mental health service providers, researchers and policy experts. A phased approach was adopted by the Commission to reach its goal, primarily focusing on what a transformed mental health system might look like (Phase 1 – completed), and secondly, on how to achieve this vision (Phase 2 – in progress).
The main goal of Phase 1 was the development and refinement of a framework document, aiming towards “Recovery and Well- Being,” and using a broad public and stakeholder engagement process including:
1) Engagement of the extended Commission: Eight permanent Advisory Committees in the Commission representing both a broad range of perspectives and Canada’s demographic and cultural diversity provided advice to the board and assisted the Commission in engaging with the broader stakeholder community. Most of the advisory committee members were individuals who were asked to contribute their personal perspectives based on their experience of mental health issues or illnesses. Additionally, there was a consumer council, comprised exclusively of people living with mental health issues.
2) Online participation Web site – public and stakeholders: A customized participation Web site was designed to collect input and opinions from the general public and stakeholder groups using open-ended and close-ended questions, as well as a free form option where the audiences could give qualitative comments. The site increased engagement due to its accessibility and privacy, and allowed the Commission to reach out to the youth, younger adults and other hard to reach groups whose voices are often unheard.
3) 12 Regional Dialogues: From February to April 2009, regional dialogues were held which brought together a cross-section of 30-40 participants, demonstrating a mix of individuals who had experienced mental health problems or illnesses, and their family members, caregivers, and policymakers, among others. Participants received the opportunity to learn about the proposed framework and provide feedback, and their full participation was encouraged.
4) Focused Dialogues: These dialogues aimed at obtaining a deeper understanding of specific needs and concerns of Canada’s aboriginal people, and of health and social services professionals to ensure they were correctly reflected in the final framework document.
5) Consultations with Federal/Provincial/Territorial Governments: The Commission integrated various meetings regarding the complexity and lasting effect of jurisdictional issues in the field of healthcare, and the need for a collaborative approach to address mental health issues. Additionally, the Commission held facilitated dialogues with members of the Canadian Public Health Network’s Mental Issue Group and a session that brought together representatives of over 10 federal departments (justice, health, etc.) to participate in dialogue on the draft framework.
A Lasting Impact
This initiative led to a complete redrafting of the framework document to reflect public and stakeholder input, including the addition of a vision statement, reframing of the goal statements and rewording of key concepts. It also signified the starting point of a new dialogue on mental health in Canada. Project evaluation results showed that the majority of the respondents and participants appreciated the opportunity to contribute to the creation of a mental health strategy and planned to stay linked with the Commission’s work to develop a strategy based on their online experience.
The Commission’s goal of moving towards a comprehensive national mental health strategy is a high-level, long-term policy objective that requires major changes in how mental health legislation, policies, programs and practices are developed and delivered by Canadian provinces and territories. The Commission will continue to involve different demographics, perspectives and regions to help raise awareness, build capacity and support advocacy to the levels necessary for sustaining a national dialogue on this critical issue, and lead decision makers to recognize and support mental health issues as a priority.
The Evolution of Therapy
Canada’s first Computer Assisted Rehabilitation Environment (CAREN) systems have been implemented in Ottawa and Edmonton to utilize Virtual Reality (VR) medical treatment systems for the care of both military and civilian patients. CAREN systems will create a secure, controlled, therapeutic learning environment for soldiers requiring physical and mental rehabilitation. It will allow participants to become part of their simulated environment and interact with it, while aiming to foster hope, provide opportunity and nurture independence for people who have faced challenges due to certain illnesses or injury.
Dr. Edward Lemaire of the Ottawa Hospital Rehabilitation Center is directly involved with the development of the system and points to ways in which the rehabilitation will affect activities of daily living. “Downtown Ottawa is now programmed into CAREN to allow people to move in their virtual community during therapy,” he says. The lab’s collaborative research is fostered by close contact with other CAREN system labs in Israel, the Netherlands and the U.S.
Canadian universities, as well, are employing VR in their labs to address healthcare concerns. Dr. Stephane Bouchard, a professor and researcher at the Université du Québec en Outaouais, focuses on the impact of cognitive behavorial therapy on anxiety disorders, and the ways in which telepsychotherapy can be delivered through video conferencing. Bouchard uses VR to study and treat a range of afflictions, from specific phobias to more complex anxiety disorders, including panic disorder and social anxiety. The work can be used for a broad range of applications and Bouchard says, “Most of the environments we develop in the lab could be used for prevention or treatment [of mental disorders].”
The Advancement of Telemedicine
Canada is leading the way for the use of telemedicine and the Ontario Telemedicine network is one of the biggest telehealth networks in the world. In 2010, the satisfaction rate of Canadian patients using telemedicine was almost 95%. Internationally, their telehealth organizations enjoy a high profile with companies operating in Latin America, Africa, Europe and the Middle East. Over 85% of Canadian telehealth companies export their products. Moreover, tele-guided surgical operations involving doctors in Canada and Japan, and Canada and France, have proved successful.
Other forms of computing technology will enhance all aspects of physical rehabilitation, Lemaire says. “This includes VR applications in the clinic, home and workplace,” he states, “wearable systems for diagnostic analysis and biofeedback; intelligent assistive devices (including smart prosthetics, exoskeletons, etc.); more intelligent wheelchair controls; and smarter outcome reporting systems to assist with clinical decision making, among others.”
While the Canadian healthcare system may be undergoing major structural changes, a bright future lies ahead for the development of health information highways and innovative telehealth applications. The research and development and export capacity of the Canadian telehealth industry shows the field is ready to offer a large range of products and services on the international market. An aging and demanding consumer will undoubtedly provide more momentum for the development of home telecare systems and more accessible health and wellness information on the Internet, in addition to diverse types of new technologies to support healthcare issues. The government’s commitment to providing its population with acceptable mental healthcare options and treatment, based on their ongoing support and input, speaks to its capacity to embrace change and the coming years will assuredly see novel, exciting developments in the field.
Sources:
Personal communication with Stephane Bouchard, Ph.D. and Edward Lemaire, Ph.D., and the World Health Organization.
AUTHORS:
Rasheda Farid & Khodeza Begum
Editorial Department
C&R Magazine
www.vrphobia.eu
editorial@vrphobia.eu
 About Brenda Wiederhold
About Brenda Wiederhold
President of Virtual Reality Medical Institute (VRMI) in Brussels, Belgium.
Executive VP Virtual Reality Medical Center (VRMC), based in San Diego and Los Angeles, California.
CEO of Interactive Media Institute a 501c3 non-profit
Clinical Instructor in Department of Psychiatry at UCSD
Founder of CyberPsychology, CyberTherapy, & Social Networking Conference
Visiting Professor at Catholic University Milan.


