





➣ By Toni Giorgino et al.
Recovery from a stroke begins in the acute unit and it is articulated into a series of intensive and extensive rehabilitation protocols. Despite the protocols variability, there is nowadays a common trend, in clinical medicine, to shorten hospitalization and foster homecare. The reason is both to cut costs and improve quality of life. The aim of My Heart’s Product Concept NR is to support patients in the performance of speech and motor therapy, both when they are still hospitalized, and after discharge, at home. Patients eligible for the service must be in stable clinical condition and show mild motor impairment and/or aphasia with no other cognitive impairment that could impact on the system’s use.
Liability constraints of Italian hospitals impose that IT-based rehabilitation does not replace conventional therapy. Therefore, at the hospital, exercise performed with the system is added to the conventional one, resulting in a more intensive, hopefully more effective, program. This could lead to an earlier discharge. After discharge, patients could bring the rehabilitation device to a long stay ward or at home, and continue exercises with the help of their caregivers.
In this paper, the service built within Concept NR will be described, in terms of its architecture, technology used and first experimental results.
The system architecture
Figure 1 shows a simplified view of the system technical architecture.
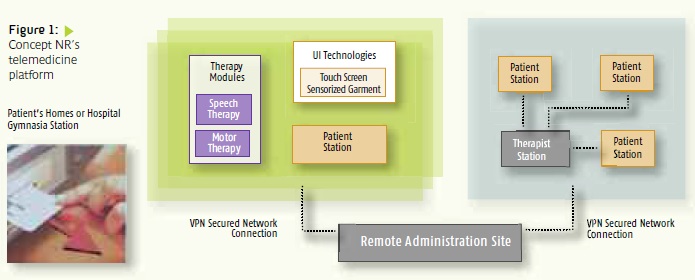
The infrastructure is based on EvoCare, a solution developed by Dr Hein GmbH. The main components are one server, and a number of users’ workstations, connected by a secure network.
Medical personnel use the therapists’ stations to administer their assigned patients, prescribe exercises, and review their performance.
Patients use the patients’ stations which support the rehabilitation exercises. Patients’ identities are recognized via per-sonal “check-in cards.” Once inserted, the exercise protocol (prepared by physicians) and messages are downloaded automatically at the patient’s site.
The server acts as the repository for exercise prescriptions, results, and messages.
Specific exercises, including speech therapy and motor therapy, are realized by a “plugin” mechanism. Each plug-in implements all activities required by the specific type of exercise: it is responsible for providing configuration screens, supports the execution of the actual exercise, provides appropriate feedback to the patient, and stores the results. It also supports browsing and summarization of the results for the therapist to review.
The technology
Speech therapy is based on the EvoLing software developed by Dr. Hein GmbH. It includes an extensive set of exercises, each promoting one ability: to recognize words, pho – nemes, graphemes, and pictures. Semantic and orthographic information is considered in order to build exercises with an adapting degree of difficulty.
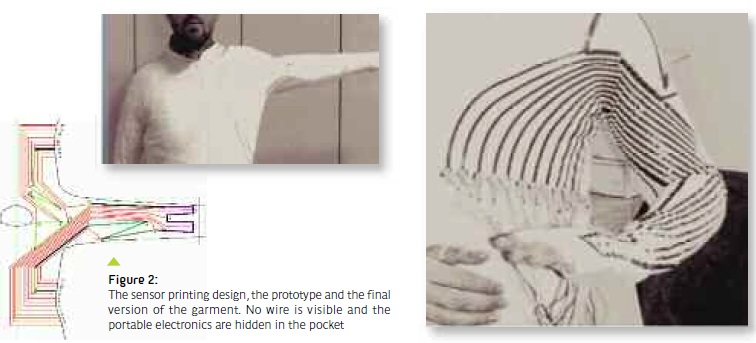
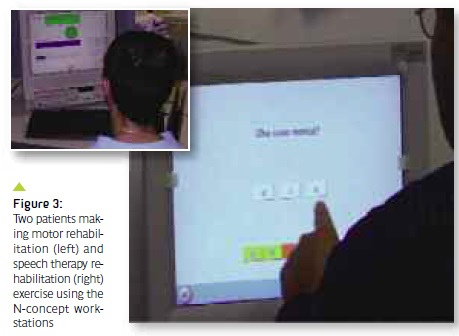
Motor therapy is an innovative component of the system. When sitting at their station, patients wear a special sensorized garment, plugged into a portable electronics box (fig. 2). After a brief calibration phase, the motion recognition software is started; it provides real-time feedback on the progress and accuracy of exercises by means of clear symbols such as colored bars and a smi l – ing/frowning face. The movements have to be repeated until the assigned number of repetitions are performed, or a timeout expires. A traffic light icon shows when to start a new repetition (fig. 3, left).
Motion recognition is based on strain sensor technology, directly printed on garments. Conductive elastomers are polymer-based materials which exhibit electrical conductivity. Sensing stripes are thin and can be printed by cheap industrial processes; they do not alter the mechanical properties of the fabric (Lycra in our case) and they are stable and nontoxic. The same material can be used to realize connection wires between sensors and the readout electronics (fig. 2).
Movement recognition
When signals from body movement are acquired, they are processed in order to verify the correct execution of the rehabilitation exercise. Since there is no direct correspondence between the fabric stretch values at various points of the garment and biomechanical parameters or like angles between limb segments, posture classification was tackled via machine-learning based algorithms. Therefore, every repetition is classified evaluating the similarity with a known “correct” or reference path. Some reference paths correspond to well-known, deficitrelated exercises, like adduction, abduction, rotation, extension, etc. But other exercises may be tailored to the specific patients, in particular functional movements like combing, eating, brushing, etc. A short “calibration session” allows the system to learn such move ments and store the corresponding reference paths.
The machine learning approach to movement recognition is an important research topic by itself, because strain sensors are affected by various sources of uncertainty, which make the recovery of limb positions from sensor readings less than straightforward. The accuracy of classification is affected by the dynamic nature of the task. Smeared sensors produce velocity-dependent artifacts; therefore, the recognition accuracy is impaired when limbs are moving. In addi-tion, patients wear the garment each time in a different way, and also within the same session the garment may slightly move. Also, one is interested in the closeness of a movement path to a reference, not just to detect a limited set of basic positions.
Results
The NR system is currently undergoing a small-scale study to assess user satisfaction and gather initial measures and feedback. It includes, in its last phase, 10 months of experience in the field, with real healthcare operators and at least 20 patients exploiting the different system functionalities. Results of the study will deal with the usability of the system (user-friendliness, lack of technical problems, comfort e.g. possible problems with the garment) and the users’ satisfaction (perceived usefulness from the patients’ and therapists’ point of view).
Preliminary qualitative and quantitative results for speech therapy were obtained from the first ten patients enrolled. Most of the enrolled patients enjoy using the system, and use it about three times a day, in addition to their traditional face-to-face encounter with the speech therapist.
Motor therapy support, while representing a very promising technology, is a more challenging task. The preliminary laboratory evaluation with voluntary subjects showed an overall efficiency on movement recognition of 91%. However, we can not report at the moment quantitative results on patients, since the first months of the evaluation phase have been spent in gathering feedback from patients (six subjects) and therapists in order to improve the system usability. The garment design has been improved adding a zip to facilitate wearing and markers to facilitate wearing the garment always in the same way. Also the interfaces have been made more and more simple and immediate, leaving out all the pictures, icons and words that could make the patient confused.
Conclusion
The integrated nature of the NR system is intended to support a multidisciplinary, telemedicine-based approach to rehabilitation. The benefits of this (and similar) ITbased aids are supported by current beliefs on rehabilitation, e.g. those expressed in the SPREAD guidelines (www.spread.it). First of all, long term rehabilitation programmes are considered beneficial for the recovery process, but cost is very high. IT technologies are a promising solution for pro-viding long-term rehabilitation at lower costs. At the same time, early discharge is recommended for patients with less severe disability. The system allows for early discharge while still being monitored remotely.
Finally, the concept addresses a frequentlyreported issue, i.e. lack of quantitative measures on the progress of rehabilitation. The diffusion of computerized monitored rehabilitation aids may increase the objectivity of practice and allow for quantitative progress evaluation and therapy comparisons.
Acknowledgments
The authors thank F. Lorussi and D. De Rossi (University of Pisa); R. Mauri (Fondazione Maugeri, Pavia); M. Stefanelli (University of Pavia); D. Tietze and R. Setz (Dr. Hein GmbH) for essential contributions to the project. The work was partly funded by EU project “MyHeart” no. IST-2002-507816.
Toni Giorgino, Ph.D.
Paolo Tormene, M.S.
Silvana Quaglini, Ph.D.
Laboratory for Biomedical Informatics,
Dipartimento di Informatica e Sistemistica,
Università di Pavia, Italy
Giorgio Maggioni, M.D.
Barbara Cattani, M.S.
Caterina Pistarini, M.D.
IRCCS Fondazione
Salvatore Maugeri, Pavia, Italy
silvana.quaglini@gmail.com
 About Brenda Wiederhold
About Brenda Wiederhold
President of Virtual Reality Medical Institute (VRMI) in Brussels, Belgium.
Executive VP Virtual Reality Medical Center (VRMC), based in San Diego and Los Angeles, California.
CEO of Interactive Media Institute a 501c3 non-profit
Clinical Instructor in Department of Psychiatry at UCSD
Founder of CyberPsychology, CyberTherapy, & Social Networking Conference
Visiting Professor at Catholic University Milan.


