





By Mark A. Neerincx
In Western society, the need for health-promoting activities of young and old citizens is increasing vastly. Assistive technologies are being developed that help to prevent or cope with chronic diseases like obesity or diabetes (which are often life-style related), and incidents like falling down or allergic reactions. By integrating social robots into these care systems, the self-care capabilities of citizens can be substantially enhanced. With contributions from different disciplines — computer, health and social sciences — various social robot applications have been developed that support self-management, e.g. for exercises, pediatrics, and autism therapy. To foster progress and application of “social robotics for self care,” coordinated efforts between research institutes, companies and end-users are being set up.
Personal Assistance in Context
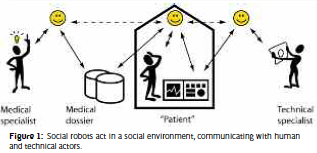 Figure 1 provides an overview of the environment of a “social robot” – it communicates with its user (“patient”) at home, the equipment and sensors in the home, the medical dossier, and other “personal agents” (e.g., medical and technical specialist). This framework was developed in the SuperAssist project on digital assistants for chronically ill, e.g. a (virtual) iCat robot to reduce the Body Mass Index of persons with obesity. Fig. 2 presents a picture of the iCat. For older adults, current research focuses on the provision of daily assistance for medication usage, healthy, regular meals, exercises for physical and mental fitness, reminders of events and activities, and warnings to avoid dangerous situations or accidents. For effective persuasion, the assistant should express social behaviors, be trustworthy and show empathy. Based on the principles from motivational interviewing and social human-technology interaction, we designed and tested a set of social robot behaviors including high-level dialogue acts (semantics, intentions), natural cues (e.g., gaze, posture), emotion expressions (e.g., compassionate face), and interaction conventions (e.g., turn taking). In an experiment on a “one-week diabetics scenario,” older adults viewed a robot character as more empathic and trustworthy than a conventional text-based assistant, and expressed more conversational behavior with the robots.
Figure 1 provides an overview of the environment of a “social robot” – it communicates with its user (“patient”) at home, the equipment and sensors in the home, the medical dossier, and other “personal agents” (e.g., medical and technical specialist). This framework was developed in the SuperAssist project on digital assistants for chronically ill, e.g. a (virtual) iCat robot to reduce the Body Mass Index of persons with obesity. Fig. 2 presents a picture of the iCat. For older adults, current research focuses on the provision of daily assistance for medication usage, healthy, regular meals, exercises for physical and mental fitness, reminders of events and activities, and warnings to avoid dangerous situations or accidents. For effective persuasion, the assistant should express social behaviors, be trustworthy and show empathy. Based on the principles from motivational interviewing and social human-technology interaction, we designed and tested a set of social robot behaviors including high-level dialogue acts (semantics, intentions), natural cues (e.g., gaze, posture), emotion expressions (e.g., compassionate face), and interaction conventions (e.g., turn taking). In an experiment on a “one-week diabetics scenario,” older adults viewed a robot character as more empathic and trustworthy than a conventional text-based assistant, and expressed more conversational behavior with the robots.
Based on these findings, we are developing and testing different robot behaviors for three scenarios – to stop wandering behavior (e.g., leaving the house in the middle of the night), to assist when a possible falldown has been detected, and to support regular drinking behavior. The research question is how to optimize the different social behaviors of the robot. It should be able to offer direction to stop wandering, ask whether the person has fallen and needs further assistance, and motivate elderly patients to drink regularly by providing friendly hints.
For children, current research focuses on the development of a “buddy” for learning routines, for improving motivation to adhere to medical recommendations, and for playing (educative) games. The ALIZ-E project started in 2010, developing methods for designing and testing interactive, mobile robots which will be able to interact with children over extended periods of time, i.e. a possibly non-continuous succession of interactions which can refer back to, and build forth on, previous experiences (EU-funded FP7 project, grant number 248116). ALIZ-E will instantiate and evaluate these methods in working systems that interact with hospitalized children undergoing diabetes treatment, using the Nao robot platform (see Fig. 4).

In conclusion, we are currently developing methods and technologies for social robots that support personal self-management and well-being on five aspects – comprehension, persuasion, resilience, mitigation and mood. Comprehension of an individual’s state is being improved, because the robot can complement automatic monitoring systems with systematic questions. Factual questions can be posed (“What time did you awake?”), as well as affective questions (“How do you feel this morning?”). Persuasion of desired behavior is being established by attuning the feedback of the robot to the patient’s general state and specific external conditions. Positive hints improve adherence to medical procedures (e.g., taking medication or blood sugar monitoring), and can be tailored to personal goals. By providing personalized medical background information, patients can be educated and coached. It can be expected that their resilience is improved by better understanding and therapy adherence. Furthermore, the information should help to cope with possible incidents, like a hypo for diabetes. When incidents are monitored, the robot can initiate or support mitigation activities, such as alarming and giving advice. Last but not least, the robot can help to improve a patient’s mood by acting as a buddy and potential actor during play games.
Mark A. Neerincx, Ph.D. Delft University of Technology The Netherlands mark.neerincx@tno.nl http://mmi.tudelf t.nl/SocioCognitiveRobotics
 About Brenda Wiederhold
About Brenda Wiederhold
President of Virtual Reality Medical Institute (VRMI) in Brussels, Belgium.
Executive VP Virtual Reality Medical Center (VRMC), based in San Diego and Los Angeles, California.
CEO of Interactive Media Institute a 501c3 non-profit
Clinical Instructor in Department of Psychiatry at UCSD
Founder of CyberPsychology, CyberTherapy, & Social Networking Conference
Visiting Professor at Catholic University Milan.