





By Giuseppe Riva
Within the healthcare domain, the European Commission focus recently shifted from the traditional hospital-centered and reactive healthcare delivery model toward a person- centered and preventive one. The main outcome of this shift is the “Personal Health Systems” (PHS) paradigm that aims at offering continuous, quality controlled, and personalized health services to empowered individuals regardless of location.
PHS cover a wide range of systems including wearable, implantable or portable systems, as well as Point-of-Care (PoC) diagnostic devices. Typically, the functioning of PHS is related to three main blocks as shown in Fig. 1.
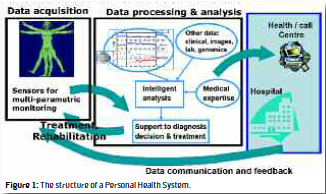
1. Data Acquisition: Collection of data and information related to the health status of a patient or healthy individual, e.g., through the use of sensors and monitoring devices.
2. Data Analysis: Processing, analysis and interpretation of the acquired data to identify what information is clinically relevant and useful in diagnosis, management or treatment of a condition. This entails processing of data at both ends – locally at the site of acquisition (e.g., with on-body electronics) and remotely at medical centers. Data processing and interpretation takes into account the established medical knowledge and professional expertise where appropriate.
3. Patient/Therapist Communication: Communication and feedback between various actors, in a loop – from patient/individual to medical center; from medical center that analyzes the acquired data to doctor/hospital; and back to the patient/individual from either the wearable/ portable/implantable system itself or the doctor or the medical center (e.g., in the form of personalized feedback and guidance to the patient, adjusted treatment via closed loop therapy, control of therapy devices).
The European Commission is supporting research in this area under the Seventh Framework Programme (FP7). FP7 funds are used to support research into monitoring systems for patients with chronic diseases. In particular, such tools should provide improved quality of life for chronically ill patients, enabling them to stay at home rather than have to be admitted to hospitals. With ICT systems able to monitor a range of parameters related to the patient’s condition, medical professionals can take timely decisions on the most effective treatment. Automatic alerts ensure doctors are immediately made aware of changes in the patient’s condition and can respond to prevent severe deteriorations.
This approach can also be used to improve mental health treatment. While most of us immediately think of either drugs or traditional talk therapy as the primary tools for mental health problems, there is a long history of using technologies for the diagnosis and treatment of psychological disorders. Specifically, PHS help us to connect on a level never seen in history, and for individuals less likely to seek professional help, they provide a confidential self-paced avenue towards change.
For these reasons, the FP7 decided to support ICT-based research projects providing solutions for persons suffering from stress, depression or bipolar disorders. These projects should address the parallel development of technological solutions, as well as new management or treatment models based on closed-loop approaches. Emphasis will be on the use of multi-parametric monitoring systems, which monitor various metrics related to behavior and to bodily and brain functions (e.g. activity, sleep, physiological and biochemical parameters).
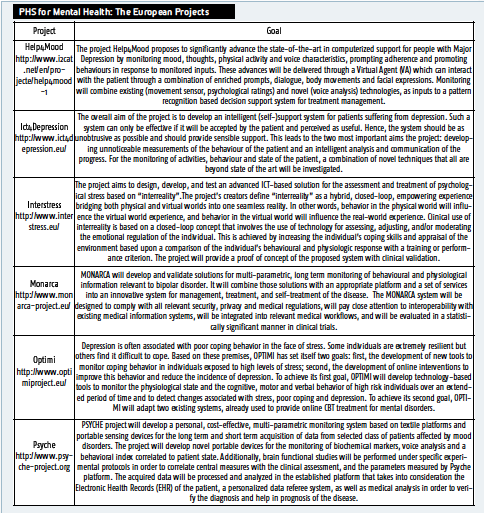
Furthermore, the required systems should aim at (i) objective and quantitative assessment of symptoms, patient condition, effectiveness of therapy and use of medication; (ii) decision support for treatment planning; and (iii) provision of warnings and motivating feedback. In the cases of depression and bipolar disorders, the systems should also aim at prediction of depressive or manic episodes. The solutions should combine wearable, portable or implantable devices, with appropriate platforms and services. Finally, they should promote the interaction between patients. After a very demanding selection, the Commission provided financial support to the following six projects – Help4Mood, Ict4Depression, Interstress, Monarca, Optimi and Psyche – that aim at using PHS based on Virtual Reality, biosensors and/or mobile technologies to improve the treatment of bipolar disorders, depression and psychological stress. A short description of their contents is in the Table. The expected end outcomes of these projects are:
• Increased mental health practitioners productivity (i.e. reduced patient unit cost through remote monitoring and self care).
• Reduced in-patient costs (i.e. due to delay of the time between when a disease becomes complex and chronic and the end of life or to the elimination altogether of the development of pre-morbid conditions into a fullblown disease);
• Decreased diagnostic and treatment costs since a lower number of visits will be needed as a result of both preventive monitoring and chronic disease management.
Giuseppe Riva, Ph.D. Istituto Auxlogico Italiano Italy giuseppe.riva@unicatt.it
 About Brenda Wiederhold
About Brenda Wiederhold
President of Virtual Reality Medical Institute (VRMI) in Brussels, Belgium.
Executive VP Virtual Reality Medical Center (VRMC), based in San Diego and Los Angeles, California.
CEO of Interactive Media Institute a 501c3 non-profit
Clinical Instructor in Department of Psychiatry at UCSD
Founder of CyberPsychology, CyberTherapy, & Social Networking Conference
Visiting Professor at Catholic University Milan.