





➣ By Giuseppe Riva

Since 1986, when the computer scientist and author Jaron Lanier used the term for the first time, “virtual reality” (VR) has been usually described as a computer simulated environment with and within which people can interact.
The basis for the VR idea is that a computer can synthesize a three-dimensional (3D) graphical environment from numerical data. Using visual, aural or haptic devices, the human operator can experience the environment as if it were a part of the world. This computer generated world may be either a model of a realworld object, such as a house; or an abstract world that does not exist in a real sense but is understood by humans, such as a chemical molecule or a representation of a set of data; or it might be in a completely imaginary science fiction world.
Further, because input devices sense the operator’s reactions and motions, the operator can modify the synthetic environment, creating the illusion of interacting with and thus being immersed within the environment. Typically, a VR system is composed by:
- the output tools (visual, aural and haptic), that immerse the user in the virtual environment;
- the input tools (trackers, gloves or a mouse) that continually reports the position and movements of the users;
- the graphic rendering system that generates, at 20-30 frames per second, the virtual environment;
- the database construction and virtual object modeling software for building and maintaining detailed and realistic models of the virtual world. In particular, the software handles the geometry, texture, intelligent behavior, and physical modeling of hardness, inertia, surface plasticity, of any object included in the virtual world.

Figure 2: Addition of haptic device on VR user’ shand to allow for “touch sensation”
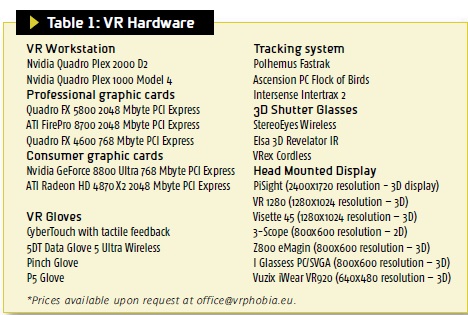
The computer technology that allows the development of three-dimensional virtual environments consists of both hardware and software (see Table 1 for VR Hardware). The computer hardware used ranges from standard PCs to high-performance workstations with parallel processors for the rapid computation of world models, and high-speed computer networks for transferring information among participants in the virtual world. The implementation of the virtual world is accomplished with software for modeling (geometric, physical, and behavioral), navigation, interaction, and hypermedia integration.
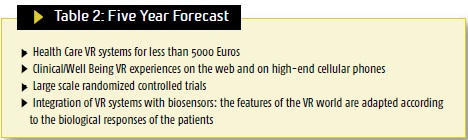
The most recent development of VR has been in the area of networking and the Internet. Networked virtual environments and 3- D interfaces to the Internet are amongst the latest applications of VR in a growing telecommunications market (See Table 2 for a 5-year forecast of VR in health care).
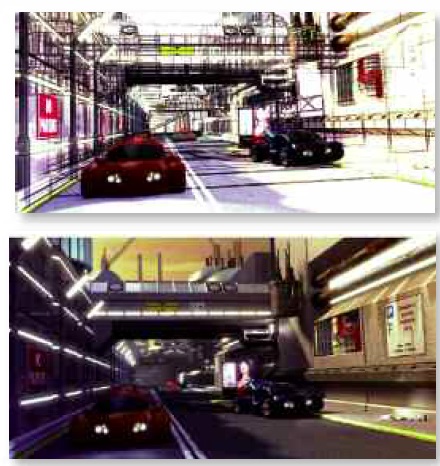
Figure 3 and 4: Examples of VR environnement before and after mapping
For many health care professionals, VR is first of all a technology. However, the analysis of the different VR applications clearly shows that the focus on technological devices is not the same in all the areas of medicine and it is related to the specific goals of the health care provider.
For instance, former Defense Advanced Research Projects Agency (DARPA) Program Manager and retired Army Colonel Dr. Richard Satava (M.D., FACS), in his recent book “Emerging Technologies in Surgery,” describes VR as: “a collection of technologies that allow people to interact efficiently with 3D computerized databases in real time using their natural senses and skills”. This definition lacks any reference to head mounted displays and instrumented clothing such as gloves or suits. In fact, less than 20% of VR health care applications in medicine are actually using any immersive equipment.
However, if we shift our attention to behavioral sciences and rehabilitation, where immersive devices are used by more than 50% of the applications, VR is described differently. For instance Drs. Brenda and Mark Wiederhold, in their book “Virtual Reality Therapy for Anxiety Disorders: Advances in Evaluation and Treatment” define VR as “an advanced form of human-computer interface that allows the user to interact with and become immersed in a computer-generated environment in a naturalistic fashion”.
These two definitions underline two different focuses of VR in medicine: VR as simulation tool and VR as interaction tool.
For physicians and surgeons, the simulation focus of VR prevails over the interaction one: the ultimate goal of VR is the presentation of virtual objects to all of the human senses in a way identical to their natural counterpart. As noted by Satava, as more and more of the medical technologies become information-based, it will be possible to represent a patient with higher fidelity to a point that the image may become a surrogate for the patient – the medical avatar. In this sense, an effective VR system should offer real life body parts or avatars that interact with external devices such as surgical instruments as near as possible to their real models. This view also drives the Informa – tion and Communications Technologies (ICT) Work Programme strategic objective “Virtual Physiological Human” (VPH). The VPH lists as its main target outcome patientspecific computer models for personalized and predictive healthcare and tools for modeling and simulation of human physiology and disease-related processes.

Figure 5: Users interacting with large scale VR environment

Figure 6: Example of Character Design software Interface
For clinical psychologists and rehabilitation specialists, the interaction focus of VR prevails over the simulation one: they use VR to provide a new humancomputer interaction paradigm in which users are no longer simply external observers of images on a computer screen but are active participants within a computer-generated three-dimensional virtual world. Within the VE the patient has the possibility of learning to manage a problematic situation related to his/her disturbance. The key characteristics of virtual environments for these professionals are both the high level of control of the interaction with the tool without the constraints usual ly found in computer systems, and the enriched experience provided to the patient.

Figure 6: Second Life online world
In the following C&R papers we discuss in more detail these two visions, describing more in detail different areas of health care in which the use of VR is actually investigated.
Both areas of VR are equally important, and equally useful, as we move towards the integration of technology into existing clinical and teaching paradigms. Technology works to assist and enhance existing clinical skills and training tools, not to replace them.
Giuseppe Riva, Ph.D., M.S., M.A.
Istituto Auxologico Italiano
www.auxologico.it/
info@auxologico.it
 About Brenda Wiederhold
About Brenda Wiederhold
President of Virtual Reality Medical Institute (VRMI) in Brussels, Belgium.
Executive VP Virtual Reality Medical Center (VRMC), based in San Diego and Los Angeles, California.
CEO of Interactive Media Institute a 501c3 non-profit
Clinical Instructor in Department of Psychiatry at UCSD
Founder of CyberPsychology, CyberTherapy, & Social Networking Conference
Visiting Professor at Catholic University Milan.